Low back pain (LBP) is a prevalent condition that affects up to 84 percent of adults at some point in their lives, with up to half of those experiencing multiple episodes. LBP has been the second leading cause of lost work days, with an estimated annual cost of $50 billion in the United States. Symptoms of LBP can range from mild to severe. Some instances of LBP seem to be self-limiting and recover without intervention, but others may be severe enough to require treatment in an emergency department. LBP can be caused by a variety of things, including muscles, nerves, bones, and referred pain from the abdominal organs. Although there are a variety of underlying factors for LBP, there is typically no one-size-fits-all solution. As a result, a greater understanding of the cause of LBP may lead to more effective solutions (Shemshaki at al, 2013).
Referred or radicular pain is the most common type of pain linked with LBP. The latter is generally referred to as sciatica, and it is distinguished by pain radiating below the knee, into the foot, and into the toes, as well as objective signs of nerve root entrapment such as sensory deficits, reflex abnormalities, and muscular weakness (Konstantinou at al, 2015). A ruptured disc, a bone protrusion on the spine, or a narrowing of the spine (spinal stenosis) compresses portion of the nerve either because of piriformis muscle or other reasons , usually causes sciatica. Inflammation, discomfort, and numbness are common symptoms in the affected leg. Though this pain associated with sciatica could be chronic, the majority of cases recover within a few weeks with non-operative therapy. People with severe sciatica who also have significant limb weakening or bowel or bladder abnormalities may be surgical candidates.
Clinical reasoning facilitates practitioners to make diagnostic assumptions based on information obtained from history taking, clinical examinations, and understanding of patients’ perspectives in order to determine therapeutic strategies and prognoses, as well as to resolve ethical dilemmas in order to assist with holistic assessments. As a result, clinical reasoning is critical to the quality of care that therapists and patients receive because it allows them to discover elements that improve functioning. This paper discusses a critical discussion of clinical reasoning and establishes a preliminary diagnosis, including pain mechanisms and flags, for a patient case study through the subjective examination of information with justifications based on research-based evidence. Further, it also suggests an objective examination plan for refuting differential diagnoses and affirming preliminary diagnoses.
Case Study
The case study patient will be referred to as Kate. She is a 36-year-old woman who experienced pain in her right buttock and knee region for nine months and had a history of the dislocated patella. 2-3 months later, the patient started feeling intermittent occurrences of deep dull pain at hip region and sharp stabbing pain at the knee region that get aggravated with prolonged sitting or bending activities. After the pain remained consistent, the patient sought physiotherapy treatment. During treatment, she responded to joint and soft tissue mobilization. She also adopted ergonomic/postural advice; a progressive active exercise programme in gym (including core stability regime). The signs and symptoms generally resolved 3-4 months ago. Residual odd “niggle” constant deep dull ache in the hip area and tightness lumbar spine still remained. Approximately 1 month ago, she started noticing a gradual increase in the frequency and incidence of aches in the posterior buttock. She noticed at work and during the commute in particular. 2 weeks ago, the pain at the hip region became intense (no particular reason) and the patient also became aware of constant sharp stabbing pain/tingling in the knee region and constant tingling in foot as well. She felt increased intensity and frequency since the onset, particularly knee pain. She is finally Unable to work last two weeks due to pain and loss of function. The patient seemed to have taken diclofenac(td) and paracetamol during the previous intervention.
Pain areas and mechanisms
In medicine, pain is the most common symptom (Merkle, Sluka & Frey-Law, 2020). Pain is an unpleasant sensation that can be broad or localized and is caused by actual or potential tissue injury. (Williams & Craig, 2016). Idiopathic, nociceptive, psychogenic, neuropathic, and mixed pain are the most common classifications. Therapeutic strategies are based on a thorough clinical evaluation of each patient’s pain situation (Cheng, 2018).
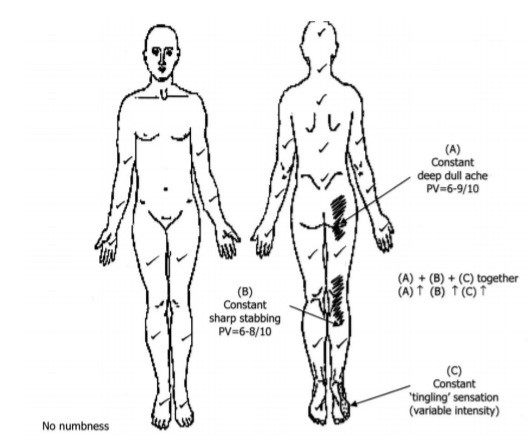
In current case study, the patient experienced pain in 3 regions; A, B and C. According to body chart, areas A and B represented, “constant deep dull ache” and “constant sharp stabbing pain” respectively, which is often related to muscle, bones pain or also nerve related pain in case of B) Shikhare, Chacko & Chuah, 2014; Mense, 2008). Kate indicated that the pain in area A persists at work and during commute in particular and progressively became more frequent with passing days. Persistent hip pain is upsetting to the patient since it impacts not only everyday activities but also quality of life. Patients frequently come with persistent lumbar spine and/or knee joint pain, making chronic hip pain challenging to diagnose. Non-orthopaedic reasons of chronic hip pain can also be involved. A good understanding of the anatomy of the hip joint and a complete history of the patient are necessary for an appropriate diagnosis of chronic hip pain (Ahuja at al. 2020).
As the patient showed a history of a dislocated patella, the previous research studies doesn’t show a link of back pain with the dislocated patella, however, the occurrence of back pain can aggravate the dislocated patella and pain in knee region as well. One study showed the beginning of sciatica has been linked to a range of occupational activities that include both mechanical stress of the hip joint (long walking and occupational lifting) and keeping a fixed posture (sitting/standing for lengthy periods). Furthermore, back pain was linked to significant repeated exposures to activities that involve repetitive usage and mechanical stress of the hip joint throughout free time (running/jogging, walking, and track and field) etc. (Pope at al, 2003). Kate signs and symptoms and work history showed that the onset of pain at A region is related to its work habits and hip joint stress. Further, the core stability regime also aggravated the pain at regions A, B, and C. Patellar dislocations may be more likely if the hip external rotators and core endurance are weak. During side plank exercise, the gluteus medius is activated, which may contribute to the large results shown in core endurance tests. Based on reliable findings, the forward step-down test could be utilized to measure dynamic weakness in hip abductors and external rotators across providers (Arnold at al, 2017).
After progressive pain at regions A and also B, the patient reported a tingling sensation in region C as well. As patient also reported the pain in region A and B increased by coughing and sneezing, so by considering the overall pain mechanism it was speculated that it occurs due to the onset of sciatica. Sciatica can cause knee pain, hip pain, and foot pain. At first the pain was existed due to work habits but due to negligence, the pain worsened due to the onset of sciatica. As one study revealed that workplace physical activity and workload, such as lifting or carrying heavy goods, have been linked to an increased risk of sciatica (Euro at al, 2019). As patient had a history of the dislocated patella, deep vein thrombosis and, most typically, brain damage are some of the consequences associated with knee dislocations. In about a quarter of all knee dislocations, neurologic injury to the common peroneal nerve would be expected to occur. The sciatic nerve splits off to form the common peroneal nerve, which runs obliquely lateral to the popliteal fossa and bends around the fibular neck. Damage to the peroneal nerve, though not a surgical emergency, can limit dorsiflexion of the foot, resulting in foot drop and gait disability. Paresthesia and sensory loss to the anterior lower lateral leg and the dorsal area of the foot seem to be also possible side effects (Median at al, 2014).
The sciatic nerve extends from your lower back to your buttocks, down the back of your thigh, and into your leg and foot. Sciatic pain may arise when this nerve gets inflamed or compressed, and it can be sensed along the full length of the nerve or across a portion of the nerve tract. This discomfort can be continuous or periodic, ranging from a mild ache to severe agony, and commonly affects the posterior hip, leg, and foot, depending on one’s regular activity. It’s difficult to distinguish sciatica from other radicular symptoms since clinical signs vary so much in practice. Physicians, on the other hand, concentrated on recognizing three types of nerve root involvement: sciatica, radiculopathy, and spinal stenosis. It simplified the differential diagnosis considerably. After considering the physical examination and based upon the hypothesis further testing were done to confirm the root cause of pain.
Flags
In physiotherapy, the ability to conduct a detailed examination of clients in order to spot red flags and create a differential diagnosis for significant illnesses is critical. In a physical therapy outpatient context, there have been no gold standard tests or assessments to verify and diagnose any suspected disorders. However, becoming able to notice the required red flags in a client’s history and physical examination is critical in order to start an urgent referral to their general practitioner or, if a physician is inaccessible, an emergency room referral (Kim at al, 2019).
The discomfort could be usually localized to one side of the body, which is one of the key red flags for identifying sciatica. Pain during standing or sitting, tingling in the legs, and stiffness or sensitivity when trying to move a leg or foot are all signs of sciatica. Sciatica is a pretty common ailment that normally goes away in 6 to 12 weeks. Giving warmth or cold to the leg, as well as pain killers and physical therapy, are all options for treatment. Surgery is needed in more extreme situations. The causes of Cauda Equina Syndrome seem to be similar to those of sciatica, with the exception that compression is applied to the cauda equina nerves at the bottom of the spine in CES. Although it has some of the similar symptoms as sciatica, there seem to be a few key differences that identify CES rather than sciatica: Back ache that is unbearable, Anesthesia for the saddle, Sexual dysfunction, bowel or bladder incontinence or retention. CES is a rare yet life-threatening medical disorder that necessitates immediate surgery to relieve pressure on the cauda equina nerves (Gardner at al, 2011).
The patient doesn’t reveal any red flags based upon the background investigations, it was perceived that she might not experience pain due to sciatica caused by CES. The sciatic nerve was perceived to be compressed due to piriformis syndrome. It frequently compresses the sciatic nerve, resulting in ipsilateral lower limb peripheral radiculopathy. Tenderness above the greater sciatic notch is common, as is symptom exacerbation with sitting and piriformis muscle stretching. Piriformis syndrome is more common in women than in males, and it usually strikes in the fourth or fifth decade of life. It can be resolved by mediation and physical therapy.
Differential Diagnosis
The patient reported of leg pain that was much worse than the back ache. Her problems worsened when she stood for long periods of time. She said her symptoms had gradually worsened over the last two weeks, with pain ranging from a 9/10 at its worst to a 5/10 at its best. Sitting for lengthy periods of time, lifting heavy objects, and twisting were all aggravating activities. Crook laying and forward bending stretches were among the relaxing practices. She also mentioned that the pain in areas A and B was impacting her walk. The most common methods for diagnosing sciatica include taking a medical history and performing a physical examination. By definition, patients complain of leg pain that radiates. They could be asked to discuss the pain’s pattern or whether it travels below the knee, and pictures could be used to assess it. Sciatica is distinguished by a dermatomal pattern of radiating pain. Patients can experience sensory issues. Neurological testing is a big part of the physical exam. The straight leg raising test, often known as Lasègue’s sign, has been the most commonly used investigation. Low back pain can occur in sciatica patients, although it is significantly lesser than the leg pain (Koes at al, 2007).
The heart exam indicated a regular pulse and rhythm, as well as normal S1/S2 with no murmurs, rubs, or gallops. Lungs seem to have been visible. Auscultation on both sides, with no extraneous sound. A neurological evaluation indicated intact light touch sensibility and +5/5 muscle strength in both the upper and lower extremities. In the bilateral biceps, patellar, and Achilles tendons, deep tendon reflexes indicated +2/4. The structural osteopathic examination showed substantial somatic dysfunction. The atlanto-occipital joint in her cervical spine had been stretched, sidebent, and rotated. C3 was flexed with sidebending and rotation to the right, and C7 was discovered to be flexed with side bending and rotation to the left after the atlanto-axial joint was turned left. On the left, counterstrain points LC1 and AC1-5 appeared tender. T5-T9 neutral, sidebent left, and rotated right all had severe thoracic dysfunction. L3-5 were neutral, sidebent right, and rotated right in the lumbar region, with a painful counterstrain point of AL1 on the right. The right side of the patient had a positive seated and standing flexion test, an anteriorly rotated innominate bone, and a sensitive inguinal counterstrain point. The patient’s right hip hurt when he flexed, abducted, or rotated internally. Sacral torsion and sensitive counterstrain sites of the right piriformis and lower pole fifth level were seen in the patient (LP5L). A short leg disparity was discovered during an examination of leg length differences.
The procedure was done after a thorough review of the patient’s medical history and a physical examination. Only individuals with “red flag” problems or who are considering disc surgery should have imaging. Therapies that were formerly passive (such as bed rest) have so far been overtaken with more active interventions (Koes at al, 2007). She reported pain till the right foot with right SLR of 40° and a stretch in the left posterior thigh at 70°. Upper motor neuron testing (Babinski, ankle clonus test, Hoffmann’s sign) indicated nothing abnormal. Serious pathologies (cancer, cauda equina) were ruled out. There was no numbness present. The pain intensified with a cough or a sneeze and the pain location aligned with the dermatomal concentration along with decreased Achilles tendon reflex in the right lateral foot. Prone knee bend test and crossed lasegue test were positive and finger to floor distance was 30cm. On palpation over the right piriformis region and PSIS, she reported mild tenderness. Her Oswestry Disability Index (ODI) score was 42% indicating severe disability. The majority of patients with radicular disorders don’t really require diagnostic imaging right away. She was advised to obtain an MRI even after this clinical info. Before moving further, I needed to make sure that the imaging findings matched the symptoms.
Clinical presentation
The L4 through S2 nerve roots make up the sciatic nerve. The big sciatic nerve in the pelvic cavity is formed by the fusion of several nerve roots. The sciatic nerve exits the pelvis posteriorly through the sciatic foramen. The nerve runs inferior and anterior to the piriformis and posterior to the gemellus superior, inferior, obturator internus, and quadratus femoris after entering the pelvis. The sciatic nerve then passes through the biceps femoris and into the posterior thigh. Finally, the sciatic nerve branches off into the tibial and common fibular nerves in the popliteal fossa behind the knee. When there is disease somewhere along the nerve’s journey, sciatica symptoms appear. Any of the disorders indicated in the differential diagnosis could be the cause of this pathology (Davis at al, 2022).
Sciatic nerve could be damage because of many reasons; including disc herniation, spinal stenosis as well as piriformis muscles. So a careful differential diagnoses is needed to know the real cause behind the pain. The piriformis muscle originally comes from the sacroiliac joint capsule on the front of the sacrum and joins to a bony knob on the femur (thigh bone) at the hip’s outermost section. The piriformis assists with external rotation and abduction of the hip, which means turning your hip outward and bringing your thigh outside to one side when your hip is flexed, such as when getting out of a car seat by raising your knee and bringing your leg out. It also provides support for walking, running, and standing. The piriformis muscle, that acts as an external rotator of the hip, is right next to the sciatic nerve. As a result, whenever the piriformis muscle gets irritated or damaged, the sciatic nerve is also affected, resulting in sciatica-like discomfort (Hicks at al, 2022).
Sciatic pain due to Piriformis syndrome is difficult to diagnose and is dependent on clinical history and presentation. Lumbar canal stenosis, disc inflammation, and pelvic reasons are all illnesses that might mirror the symptoms of piriformis syndrome. The piriformis muscle (PM) arises from the pelvic surface of sacral segments S2-S4 in the areas between and lateral to the anterior sacral foramina, the sacroiliac joint (superior margin of the greater sciatic notch), the anterior sacroiliac ligament, and, on rare occasions, the anterior surface of the sacro-tuberous ligament. It inserts onto the greater trochanter of the femur after passing through the greater sciatic notch. External rotation, abduction, and partial extension of the hip are all functions of the PM (Chapman at al, 2012).
Symptoms of piriformis syndrome include recurrent and radiating low back pain, (chronic) buttock pain, numbness, paraesthesia, difficulties walking, and other functional tasks such as pain with sitting, crouching, standing, and bowel motions, as well as dyspareunia in women with severe cases. In virtually all cases, they could also have pressing pain in the buttock along the same side as the piriformis lesion, as well as point sensitivity above the sciatic notch. The pain in the buttocks might spread to the hip, the back of the thigh, and the proximal part of the lower leg. Activity, prolonged sitting or walking, squatting, hip adduction and internal rotation, and manoeuvers that enhance the strain of the piriformis muscle could aggravate pain. Neurological abnormalities characteristic of a radicular syndrome, such as decreased deep tendon reflexes and myotomal weakening, do not exist in piriformis syndrome. While walking, the patient may have a limp or a shortened, externally rotated leg (Hopayian at al, 2010).
Based on which nerve is injured due to piriformis syndrome, sciatica symptoms of paresthesia or dysesthesias, as well as oedema in the lower leg, may vary. Pain, tingling, and numbness in the thigh are symptoms of the L4 nerve being crushed or inflamed. When stretching the leg, the sufferer feels weak and could have a weak knee jerk reflex. Pain, tingling, and numbness may spread to the foot and big toes when the L5 nerve is crushed or inflamed. Pain, tingling, and numbness on the outer area of the foot occur when the S1 nerve is crushed or inflamed. When the patient lifts his heel off the ground and stands on his tiptoes, he feels feeble. The ankle jerk reflex could be affected.
Kate demonstrated a number of risk factors for acute pain sciatica. Intrinsic risk factors included the following:
- Age: Sciatica pain is more frequent in people between the ages of 30 and 55.
- Weight: Overweight people are more likely to experience back pain.
- Reproduction cycle: Hormonal changes after menopause raise the risk of disc damage.
The following were discovered to be extrinsic risk factors:
- Mechanism: Muscle spasm of the piriformis muscle, caused by stimulation of the muscle or a neighbouring structure such as the sacroiliac joint or hip.
- Workplace demands; extended sitting puts severe compressive stresses on the piriformis muscles.
- Posture: Using a laptop for work that isn’t properly set up might put a lot of strain on the piriformis muscles and sciatic nerve.
The patient’s functional capabilities were investigated first, as they can reveal many deficits including pain provocation, motor control techniques, confidence, and protective behaviors. Kate was slouching in her chair, Pace’s sign is discomfort and weakness caused by resisted abduction and external rotation of the hip. A positive result was found, indicated the occurrence of piriformis syndrome. Hip flexion (indicating TFL shortening) and/or leg external rotation (indicating piriformis shortening) and/or ‘hiking’ of the hip occurred at the start of the action during the Hip abduction test (indicating quadratus overactivity and therefore, by implication, shortness). She also showed Freiberg sign that involved pain and weakness when the hip was passively forced internally rotated in the supine position. The pain was assumed to be caused by piriformis muscle passive stretching and pressure on the sciatic nerve at the sacrospinous ligament.
Although lumbar palpation as a single clinical test has low inter-rater reliability and diagnostic accuracy, palpation procedures that cause a reproduction of symptoms in association with clinical reasoning can be helpful in diagnosis and as a re-assessment marker. During palpation of the larger sciatic notch, the sacroiliac joint, or the piriformis muscle belly, Kate experiences sensitivity. The spasm of the PM was detected with thorough, deep palpation. There appeared discomfort and pain with high digital palpation in the gluteal and retro-trochanteric areas, as well as an exacerbation of tightness and leg tingling. To determine the cause of the sciatic pain, an MRI of the right hip and pelvis was conducted. The axial and coronal oblique planes, which are perpendicular and parallel to the sacrum bone, were used to obtain MRI images. An MRI revealed a split piriformis muscle and a posterior aberrant slip of the sciatic nerve, which travelled through the split muscle bellies. Thus the detailed objective examination of patient and clinical testing revealed the presence of sciatic pain due to Piriformis syndrome.
Management
Davis (2022) stated that even if no medical treatment is taken, most episodes of sciatic pain improve in less than 4 to 6 weeks with no long-term problems. The patient’s recovery may take longer in more severe situations or when a neurologic disability was present. However, the prognosis for recovery seems to be quite good. Low occupational mechanics, psychological depression, and poor socioeconomic conditions have all been linked to an increased risk of chronic, recurrent sciatica, according to certain studies. Using hot or cold packs for ease and to reduce inflammation, avoiding inciting tasks or prolonged sitting/standing, practicing good, erect posture, participating in exercises to increase core strength, slight stretching of the lumbar spine and hamstrings, regular light exercises – for example walking, swimming, or aquatherapy, and using proper lifting techniques are all common ways to manage sciatica.
Medical interventions include short course of oral NSAIDs, opioid and nonopioid analgesics Muscle relaxants, anticonvulsants for neurogenic pain, in the event oral NSAIDs are insufficient, a course of oral corticosteroids may be beneficial, localized corticosteroid injections, spinal manipulation, deep tissue massage may be helpful, physical therapy consultation, surgical evaluation and correction of any structural abnormalities such as disc herniation, epidural hematoma, epidural abscess, or tumor and acupuncture (Davis, 2022).
Almost all piriformis syndrome treatment plan would include an emphasis on stretching the piriformis muscle cautiously and gradually. The patient was hospitalized for few days and was administrated few medications to help relieve pain. Rather of doing general exercises, I suggested her to ease into the physical activities she enjoys the most. We chose to start lightly with walking and exercise therapy because it was her favorite activity. We set small goals in terms of minutes walked and gradually increased the intensity as she improved and gained confidence. Painting became a stress reliever for her, so we gradually added it to her stress management strategy. After some recovery, ergonomic education was used to improve work positions that would lessen posterior annulus compression. Kate was given a lumbar roll, which had been shown to be effective in facilitating this transition. Confirmation was also given in an effort to calm her fears about her work and exercise constraints, which is crucial in improving health outcomes. Kate said she felt more at ease at work after a two-day follow-up (sitting tolerance 45 minutes). Physiotherapy of central mobilization of L4 improved lumbar flexion substantially, and evaluation revealed that Pa had stopped. Pb in flexion and PSLR improved after L5 mobilization and repeated extension in lying (REIL). These approaches were chosen because Kate’s symptoms were relieved by relative extension, as determined by a physical examination; each technique was utilized to introduce relative extension to the region. Her rehabilitation treatment comprised exercises to improve motor control, dynamic muscle strengthening, and directional preference exercises, as well as neurodynamic mobilization.
As she began to enjoy ‘staying active,’ the patient discovered that workouts proved safe for her. She stated that the neurodynamic sliders “worked well for her” in terms of pain management independence. After some time, she stated that her discomfort had decreased to a 5/10 and that she had been walking more. She was able to sit and paint for 30 min after she stopped taking her meds. She reported 2/10 leg soreness and being self-sufficient with her exercises a few weeks later. She stated that, while her symptoms did not totally resolve, she could tell that she had made significant improvement and that she found the rehab plan to be very beneficial. She experienced pain-free active range of motion in her leg and improved movement after following the therapeutic regimen. She was able to walk for 5 kilometers without pain and sit at work without discomfort. The patient was hopeful to recover further if stick with the management plan.
Conclusion
In conclusion, this study discusses the importance of clinical reasoning, which is central to the quality of care and practices. The study also addresses how to determine a preliminary diagnosis based on the subjective examination and setting a plan for objective examination to confirm a preliminary diagnosis.
After analyzing the subjective data for Kate’s case, the potential diagnosis is sciatic nerve compression due to piriformis syndrome and previous medical history. Therefore, to confirm Kate’s case, several approaches were chosen to identify and distinguish his preliminary diagnoses, such as general observation, measurement of his range of motion and quality of movement, palpation, and special tests.
Appendix
Clinical reasoning planning sheet
- List (in order of likelihood) all possible structures/tissue that could be responsible for each of the patient’s symptomatic area(s).
| List structures/tissues in order of priority | Reasons |
| Sciatic nerve | Between the linked muscles of the thigh, the sciatic nerve travels downward. From the pelvis to the knee, it is encased in a single continuous fatty sheath. The nerve splits into two branches at the knee. These branches extend into foot. So depending on overall symptoms, it was inferred that sciatic nerve might be affected. |
| L5-S1 | L5-S1 helps transfer loads from the spine into the pelvis and legs. |
| Peroneal nerve | The peroneal nerve is a branch of the sciatic nerve, which supplies movement and sensation to the lower leg, foot and toes. |
| Piriformis Muscle | The sciatic nerve is irritated by the piriformis muscle, which produces pain in the back of the leg and foot. In virtually all cases, they can also have pressure pain in the buttock on the same side as the piriformis lesion, as well as point sensitivity above the sciatic notch. The pain in the buttocks might spread to the hip, the back of the thigh, and the proximal part of the lower leg.
|
1.2 what’s the irritability of patient’s condition?
The pain often makes it difficult to sleep, leading to fatigue and irritability during work. It could be modest or burst into a throbbing ache that clutches the back and leg and makes even the smallest movement unbearable. Moving, coughing, or sneezing aggravates the symptoms. Activities that put pressure on the sciatic nerve, like bending forward from the waist or flexing the hips while the knees are straight, might make symptoms worse.
- what’s the severity of this patient?
Moderate: If you have “sciatica,” you’ll feel pain anywhere along the sciatic nerve’s course, which runs from the lower spine to the hips, buttocks, and/or down your legs. It could also produce leg and foot muscular weakness, paralysis, and a tingling pins-and-needles sensation in your leg, foot, and toes. Sciatica could be severe if your pain lasts longer than a week, or becomes progressively worse. Sufferers should get immediate medical care if: have sudden, severe pain in your low back or leg and dysfunction or muscle weakness in the leg. The numbness in severe case can lead to permanent disability.
- what’s the degree if disability?
Moderate: The term “sciatica” commonly refers to the sciatic nerve’s neuralgia (a sharp pain caused by an inflamed or injured nerve). As a result, neuralgia is the most common symptom among veterans; yet, a veteran’s sciatica may appear with symptomatology associated with a higher level of severity. The patient showed 20% neuralgia of sciatic nerve which means moderate neuralgia; characterized by tingling, numbness, and moderate to severe pain, as well as impairment in the function of the affected limb.
- Identify the tissue mechanism present?
The tissue involves in pain mechanism the sciatic nerve, peroneal, foot intrinsic, and Hip Ext Rot. Walking, jogging, climbing, lifting weights, and standing are all possible thanks to the mixed (sensory and motor) sciatic nerve, which provides the majority of functions in the lower limbs.
A healthy sciatic nerve is well covered by the buttock muscles at its origin and cannot be palpated (felt by touching or pressing on the skin. However, if the sciatic nerve is damaged, the leg may feel tight and inflexible when moving. The nerve can cause debilitating pain, weakness, and tingling in the lower back, buttocks, and leg when it is irritated or impinged.
- Identify the dominant pain mechanism present?
The dominant pain mechanism is related to sciatic nerve which is characterised by pain that extends from your lower (lumbar) spine to your buttock and down the back of your leg.
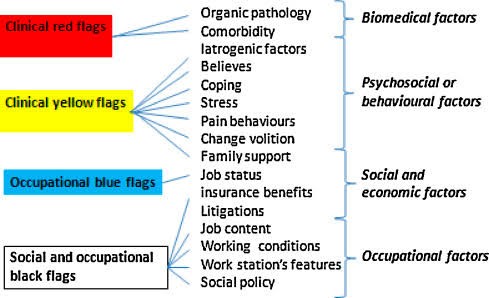
- Identify any potential risk factors (including red, yellow, blue and black flags) which may be counterproductive to recovery. Please justify
The patient doesn’t show any red flag risk factors. However, there is instances of yellow flags that can be recovered through medication and physiotherapy. The potential risk factors associated with red, yellow, blue and black flags are as follows;
- Is this disorder suited to further objective examination? YES / NO
No
If NO please identify if there is a need to examine other factors (e.g. red flags, yellow flags)
Yes, there is need to examine red and yellow flags in addition to patient’s history and physical examination so that treatment plan can be adopted correctly.
- Is there any indication for caution in undertaking the objective examination? YES / NO
If YES, please justify.
No
1.10 From questions (1.2 to 1.9) will you need to modify your objective examination? YES / NO
If YES, how will it be modified?
No
1.11 What MUST you test on day 1?
First of all, patient will be asked for physical test. She will be asked to walk during your physical exam to see how her spine carries her weight. To test the strength of her calf muscles, she will be instructed to walk on her toes and heels. Then there will be a straight leg raise exam. She will lie on her back with her legs straight for this test. She’ll be asked to slowly elevate each leg and mark the spot where the pain starts. This test helps to pinpoint the nerves that are impacted and identifies if one of her discs is damaged. She will be asked to perform more stretches and activities in order to localize pain and assess muscle flexibility and strength.
1.12 What SHOULD you test in the future?
I may prescribe medical imaging or diagnostic nerve block studies if sciatica is suspected. These tests are done to determine what is causing your sciatica. Medical imaging and diagnostic injections can also aid in the planning of surgeries and other invasive procedures.
1.13 What COULD you test in the future?
If it’s possible she has a herniated disc/ spinal stenosis/piriformis syndrome that’s causing her sciatica, I may order a magnetic resonance imaging (MRI) test or discogram test.
1.14 What differential diagnoses should you bear in mind that may have to be investigated?
Around 85% of cases are caused by a herniated lumbosacral disc crushing a nerve root, most typically at L4-L5 or L5-S1. Spinal stenosis, spondylolisthesis, cauda equina syndrome, compression by pelvic tumors, trauma, and piriformis syndrome are among the other causes. Considering the patient’s medical history, the differential diagnosis will be done for herniated discs, or when a disc protrudes, irritating the nerve root, sciatica, degenerative disc disease, bone spurs, tumors in the spine etc.
1.15 From the history, what are your objective findings likely to be?
As patient showed the history of dislocated patella, the previous research studies doesn’t showed the link of back pain with dislocated patella, however the occurrence of back pain can aggravate dislocated patella and pain in knee region as well. So, the beginning of sciatica has been linked to a range of occupational activities that include both mechanical stress of the hip joint (long walking and occupational lifting) and keeping a fixed posture (sitting/standing for lengthy periods). Furthermore, back pain was linked to significant repeated exposures to activities that involve repetitive usage and mechanical stress of the hip joint throughout free time (running/jogging, walking, and track and field) etc
1.16 What information from the history could be useful in measuring the effectiveness of the management regime chosen?
In previous history showed by client, she sought physiotherapy treatment after the pain remained consistent. During treatment she responded to joint and soft tissue mobilization. She also adopted ergonomic/postural advice; progressive active exercise programme in gym (including core stability regime). The signs and symptoms generally resolved 3-4 months ago. So such regime can be useful in measuring the effectiveness of management regime chosen.
1.17 What is your preliminary diagnosis (including tissue and pain mechanisms)?
A history and physical examination were used to make a preliminary diagnosis for the patient. Radiating leg pain was stated by the patient. She was asked to describe the pain’s distribution and whether it radiates below the knee, and she was asked to illustrate the pain’s distribution. Sciatica is distinguished by radiating pain with a dermatomal pattern. Patients were asked to report any sensory complaints they were experiencing.
Reference
Shemshaki, H., Nourian, S. M., Fereidan-Esfahani, M., Mokhtari, M., & Etemadifar, M. R. (2013). What is the source of low back pain? Journal of craniovertebral junction & spine, 4(1), 21–24. https://doi.org/10.4103/0974-8237.121620
Konstantinou, K., Dunn, K. M., Ogollah, R., Vogel, S., Hay, E. M., & ATLAS study research team (2015). Characteristics of patients with low back and leg pain seeking treatment in primary care: baseline results from the ATLAS cohort study. BMC musculoskeletal disorders, 16, 332. https://doi.org/10.1186/s12891-015-0787-8
Merkle, S. L., Sluka, K. A., & Frey-Law, L. A. (2020). The interaction between pain and movement. Journal of hand therapy: official journal of the American Society of Hand Therapists, 33(1), 60–66. https://doi.org/10.1016/j.jht.2018.05.001
Williams, A., & Craig, K. D. (2016). Updating the definition of pain. Pain, 157(11), 2420–2423. https://doi.org/10.1097/j.pain.0000000000000613
Cheng, S. T., Leung, C., Chan, K. L., Chen, P. P., Chow, Y. F., Chung, J., Law, A., Lee, J., Leung, E., & Tam, C. (2018). The relationship of self-efficacy to catastrophizing and depressive symptoms in community-dwelling older adults with chronic pain: A moderated mediation model. PloS one, 13(9), e0203964. https://doi.org/10.1371/journal.pone.0203964
Lahrach, K. & Abdulrazak, S. & Marzouki, Amine & Boutayeb, Fawzi. (2019). Surgical management of intramuscular hemangioma of the foot: A case report. Patient Safety in Surgery. 13. http://doi.org/10.1186/s13037-019-0197-1.
Mense S. (2008). Muscle pain: mechanisms and clinical significance. Deutsches Arzteblatt international, 105(12), 214–219. https://doi.org/10.3238/artzebl.2008.0214
Ahuja, V., Thapa, D., Patial, S., Chander, A., & Ahuja, A. (2020). Chronic hip pain in adults: Current knowledge and future prospective. Journal of anaesthesiology, clinical pharmacology, 36(4), 450–457. https://doi.org/10.4103/joacp.JOACP_170_19
Pope, D. P., Hunt, I. M., Birrell, F. N., Silman, A. J., & Macfarlane, G. J. (2003). Hip pain onset in relation to cumulative workplace and leisure time mechanical load: a population based case-control study. Annals of the rheumatic diseases, 62(4), 322–326. https://doi.org/10.1136/ard.62.4.322
Arnold, S., Bradshaw, E., Hansen, A., Knutson, J., and Newman, M. (2017). The Influence of Hip Strength and Core Endurance on Recurrent Patella Dislocations: A Pilot Study. Retrieved from Sophia, the St. Catherine University repository. https://sophia.stkate.edu/dpt_papers/61
Euro, U., Heliövaara, M., Shiri, R., Knekt, P., Rissanen, H., Aromaa, A., & Karppinen, J. (2019). Work-related risk factors for sciatica leading to hospitalization. Scientific reports, 9(1), 6562. https://doi.org/10.1038/s41598-019-42597-w
Medina, O., Arom, G. A., Yeranosian, M. G., Petrigliano, F. A., & McAllister, D. R. (2014). Vascular and nerve injury after knee dislocation: a systematic review. Clinical orthopaedics and related research, 472(9), 2621–2629. https://doi.org/10.1007/s11999-014-3511-3
Koes, B. W., van Tulder, M. W., & Peul, W. C. (2007). Diagnosis and treatment of sciatica. BMJ (Clinical research ed.), 334(7607), 1313–1317. https://doi.org/10.1136/bmj.39223.428495.BE
Kim Y. J. (2019). Red flag rules for knee and lower leg differential diagnosis. Annals of translational medicine, 7(Suppl 7), S250. https://doi.org/10.21037/atm.2019.07.62
Gardner, A., Gardner, E., & Morley, T. (2011). Cauda equina syndrome: a review of the current clinical and medico-legal position. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 20(5), 690–697. https://doi.org/10.1007/s00586-010-1668-3
Davis, D., Maini, K., & Vasudevan, A. (2022). Sciatica. In StatPearls. StatPearls Publishing.
Hicks, B. L., Lam, J. C., & Varacallo, M. (2022). Piriformis Syndrome. In StatPearls. StatPearls Publishing.
Chapman, C., & Bakkum, B. W. (2012). Chiropractic management of a US Army veteran with low back pain and piriformis syndrome complicated by an anatomical anomaly of the piriformis muscle: a case study. Journal of chiropractic medicine, 11(1), 24–29. https://doi.org/10.1016/j.jcm.2011.06.011
Hopayian, K., Song, F., Riera, R., & Sambandan, S. (2010). The clinical features of the piriformis syndrome: a systematic review. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 19(12), 2095–2109. https://doi.org/10.1007/s00586-010-1504-9